

Decades of intensive experimental and clinical research have revealed a great deal about how the human heart works. Though incomplete, this knowledge has been used to construct computer models that represent the activity of this organ as a whole, and of its individual chambers, the atria and ventricles, down to its tissues and cells. Such models have been used to better understand life-threatening irregular heartbeats; they are also beginning to be used to guide decisions about the treatment of patients and the development of new drugs by the pharmaceutical industry.
Yet existing computer models of the electrical activity of the human heart are sometimes inconsistent with experimental data. This issue led Dr Jakub Tomek, now a Postdoctoral Researcher in DPAG, to try and find an answer to this problem during his tenure in the Department of Computer Science as part of Professor Blanca Rodriguez’s Computational Cardiovascular Science Team. At the start of the project, the team observed that the most popular computer model at the time predicted a large increase in cellular contractility in response to sodium blockade, which is not compatible with clinical and experimental data. “This observation made us start working on a new model, but in the end, the journey towards success was much longer and more complicated than we initially expected.” (Dr Tomek).
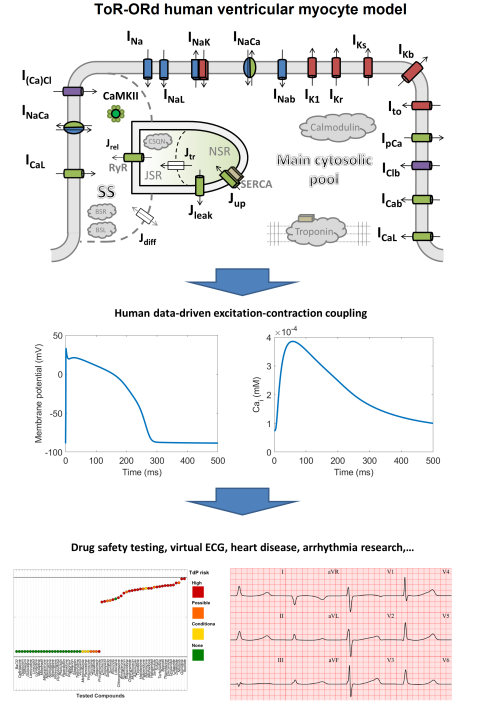
Dr Tomek and Prof. Rodriguez led new research with the aim of creating a new model that could recreate the electrical activity of the ventricles in a human heart, and that crucially would be consistent with established biophysical knowledge and experimental data for a wide range of conditions including disease and drug action. The result of this work is a model representing membrane potential, ionic currents, fluxes, and ionic concentrations in multiple areas of a myocyte, a heart muscle cell. These processes are modelled using sets of differential equations that are constructed based on experimental measurements.
The standard approach to development of computer models is to build and change a model until it fits a set of experimental data. “However, in our experience, when making any changes to a model to improve it, it is common that other properties of the model stop working that well. If a model developed to agree with a set of experimental data is consistent with them, is it because it is genuinely plausible, or is it because all its problems are in properties one does not look at? Can we trust the predictions of such a model?” (Dr Tomek).
To avoid these previous pitfalls of model creation, the team designed a strategy that split the development process of calibration and construction of the model from its validation. First, they developed the model to explicitly fit selected calibration criteria that covered a broad range of key fundamental properties of cardiomyocyte excitation-contraction coupling, the process that causes the heart to contract and pump blood out. Following this, they validated their developed model on data that was not used in the model construction, to include properties such as the response to remodelling present in cardiac disease.
The new validation data pushed our model outside its comfort zone, and it performed very well in scenarios for which it was not designed, so we believe the model is getting many fundamental properties right. - Dr Tomek
The validation ultimately showed the model was able to integrate and explain a wide range of properties of both healthy and diseased hearts, including their response to different drugs. While most of the work has focussed on thorough validation of single-cell behaviours, more cells can be coupled to form sheets of tissue or 3D structure of the heart, enabling study of spatial patterns of arrhythmia, or even understanding of how cardiac abnormalities manifest on the ECG. The team hopes that their new human heart model will enable more basic, translational and clinical research into a range of heart diseases and accelerate the development of new therapies.
Dr Jakub Tomek said: “Our model is one of the few which are based on data from human myocytes and hearts. Given important species differences between mammals, this makes our model well-suited for translational studies, such as drug safety testing, compared to animal-based models.
Compared to previous state-of-the-art human computer model, it has a very accurate shape of electrical activation, and it responds well to sodium blockers with regards to contractility. While these properties sound quite simple, the fact that we could achieve an all-around data-consistent model required reformulation of basic biophysical properties of the L-type calcium current, substitution of multiple formulations of ionic currents (including hERG), and use of artificial evolution to produce a model that would tick all the boxes we asked it to do.”
“We think there are three pillars on which this project stands. First, the model itself is a success with regards to how much human data it agrees with, and that it could predict behaviours for which it was not designed. Second, we hope the strategy of separate calibration and validation will become a standard in developing trustworthy models. This could be aided by the fact that we freely provide a model-evaluation tool which simulates a wide range of protocols and visualises the results, enabling rapid assessment of newly developed models. Third, while developing the model, we made several theoretical observations on modelling the L-type calcium current and hERG, which are broadly relevant for cardiac simulations and that suggest important improvements that are likely to be reflected in future models developed in the field.”
“The model will be a useful tool for basic and translational research of myocyte electrophysiology and excitation-contraction coupling, particularly in humans. It can be used as a platform to represent cardiac disease, and/or pharmacological therapy. Its performance in drug safety prediction suggests it’s a highly promising tool for this purpose and we already see an interest from the pharmacological industry. Ultimately, while the basic model represents a single cell, it can be connected into 2D sheets of simulated tissue or even 3D hearts including their structure derived from MRI. This opens possibilities of research into spatial patterns of arrhythmia, or prediction of which sites to ablate in clinical setting. A near-future work will be to integrate the model with computer models of contraction, which will enable studies on cardiac contractility, for example, how it is modulated by cardiac structure, disease, or therapies.”
The full paper ‘Development, calibration, and validation of a novel human ventricular myocyte model in health, disease and drug block’ can be read in eLife Sciences.